Improved Quality of Health Care Does Equate to Lower Costs
November 4, 2016
STANDARD CARE PROTOCOLS WERE OBSERVED TO BE EFFECTIVE IN IMPROVING CARE QUALITY AND REDUCING COST IN A STUDY COMPARING QUALITY AND COST OUTCOMES WITH AND WITHOUT THE USE OF SUCH PROTOCOLS.
Over the past decade, hospitals have been implementing process and quality improvement programs using strategies proven in other industries to solve their complex challenges. A primary focus of these efforts has been to identify standard care protocols that can contribute not only to improved outcomes but also to reduced costs.
These efforts raise two important questions that should be of interest to finance leaders of hospitals and health systems:
- What is the most effective methodology for identifying such standard care protocols?
- What actual evidence exists to show that such protocols are actually effective in improving outcomes and reducing costs?
Improving Care Processes: The Lean Approach
One methodology for identifying standard care protocols that has been widely adopted is lean. The Cambridge-Mass.-based Lean Enterprise Institute describes lean as a system that seeks to increase value for customers with fewer resources by eliminating waste or steps that do not add value.
Lean changes thinking at the levels of both the organization and the individual. In lean, a reviewer examines every step in a process, asking whether the step is in any way valuable to the customer. If the step lacks any apparent value, the next question is whether it can be eliminated or—if eliminating it is not possible—whether the amount of time spent on it can be reduced. In a hospital setting, the customer is the patient.
Using lean to examine hospital processes provides a broader perspective than can be gained from simply looking at processes occurring in just one department. A lean reviewer follows every step that a patient encounters with the organization, looking at the patient’s experiences across departments, specialties, and cross functional teams. A lean team then collaborates to redesign processes to make them more efficient (remove waste) and effective (add value).
The reviewer should be someone who is trained in lean. In a hospital, it could be someone in process improvement, quality, project management, or operations management. Team members would be any individuals who are involved in the steps in the process. If the process is making check-in more efficient, for example, then the team members should be from patient access and registration—ideally from the department where the change is occurring. If the process is focused on making changes to order sets, then the team should include clinical experts, physicians who will be entering orders, and other parties affected, such as representatives from pharmacy, nursing, and ancillary service areas.
Such a practice aligns with the intent of the Centers for Medicare & Medicaid Services (CMS) in advancing Medicare alternative payment models (APMs). CMS is developing programs in which hospitals are paid on the basis of the value of the care they deliver, rather than the volume of that care. The essential idea underlying the Comprehensive Care for Joint Replacement (CJR) model, for example, is to view a clinical episode from the patient’s perspective. The CJR model is testing a way to bundle payment and quality measurement for an episode of care associated with hip and knee replacements with the larger goal of encouraging hospitals, physicians, and post-acute providers to work together to coordinate care and increase value. Hospitals also have an incentive to reduce patient complications (improve quality and value) and reduce costs (minimize waste) associated with the episode of care. Using lean practices, therefore, may offer one of the best means for hospitals to begin to grapple with managing such APMs.
As processes are viewed and revamped from a lean perspective, the new process developed should then be used consistently with every customer. The idea of promoting this level of standardization of work in health care may seem counter-intuitive, given that it is the individual who is most valued in health care, with the inherent understanding that each patient is unique and has unique needs. Moreover, physicians are valued, first and foremost, for their ability to diagnose and treat each patient’s unique symptoms and needs. Decision-making at the individual level therefore is important. Nonetheless, it also stands to reason that if a process is clearly identified as being the best, there is a sound rationale for adopting it as standard practice.
As was suggested previously, lean is a useful methodology in a hospital setting for the development of standard care protocols, including standard order sets. When developed with cross functional teams and clinical expertise, standard order sets identify the best way for a physician to treat a patient and minimize waste. By enabling physicians to find all orders needed for treatment in one place, instead of having to search for and sign single orders multiple times, standard order sets not only improve efficiency but also allow for best practices on clinical care pathways to be presented in an actionable way.
Case Study: Effectiveness of Standard Order Sets
Standard order sets have been widely touted as an effective means to improve patient outcomes and reduce costs for organizations. Until recently, however, that claim has been difficult to prove.
To assess the effectiveness of standard order sets and their impact on cost and quality, a study was performed examining compliance with core measures and standard order sets at a 1,000-bed hospital in the southeastern United States. This study’s findings corroborate what has long been suspected: that standard treatment protocols do correlate with better patient outcomes and reduce waste (cost) for the organization.
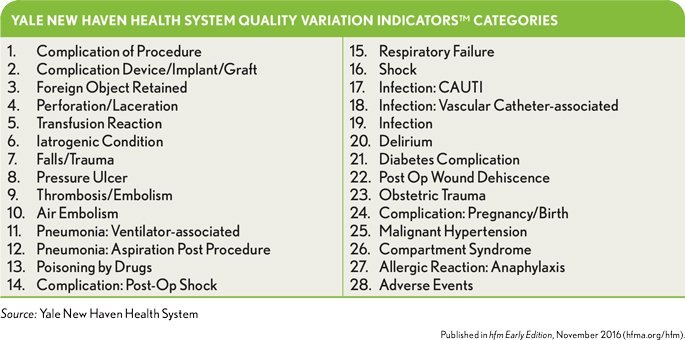
The study reviewed core measure order set compliance for acute myocardial infarction (heart attack), heart failure, hemorrhagic stroke, pneumonia, sepsis, and stroke. Quality outcomes were assessed using Yale New Haven Health System’s Quality Variation Indicators™ (QVI) methodology. QVIs are defined as potentially preventable adverse events occurring in inpatient encounters that, with the exception of surgical site infection, are not present on admission.
There are 28 QVI categories with 65 specific QVIs ranging from respiratory failure, to ventilator-associated pneumonia, to postoperative wound dehiscence.
QVI outcomes were used because they are more comprehensive than other outcome measures available, including the Agency for Healthcare Research and Quality (AHRQ) Patient Safety Indicators (PSIs). For example, AHRQ PSI 12 Perioperative Pulmonary Embolism (PE) or Deep Vein Thrombosis (DVT) Rate measures only PEs and DVTs affecting surgical inpatients. By contrast, the Thrombosis QVI captures all PEs and DVTs occurring during an inpatient stay (surgical, medical, and obstetric).
The Findings: Quality
The hospital identified nearly 9,000 inpatient encounters over a one-year period that qualified for the use of one or more of the core measure standard order sets. In actual practice, only 30 percent of these 9,000 (about 2,700 patients) received standard care protocols via an established treatment order set. The study found that, of the 9,000 patients, 14.5 percent (about 1,300 patients) had acquired one or more preventable adverse events (QVIs) during their inpatient visit.
When the patients were stratified, it was found that 16 percent of patients who did not receive the appropriate core measure order set acquired one or more QVIs, whereas only 11 percent of patients who received the appropriate core measure order set acquired one or more QVIs. This finding suggests a patient who is not treated using the appropriate core measure standard care protocol has a greater likelihood of acquiring one or more QVIs during an inpatient stay than a patient who undergoes this treatment protocol (p-value < 0.0001).
The Findings: Cost
In examining costs for the same 9,000 patients, patients who did not receive treatment using the appropriate core measure standard care protocol incurred significantly more costs than did patients who received treatment under the appropriate core measure order set (p-value < 0.0001). The average direct variable cost per case for those patients whose treatment did not follow the standard care protocol was $11,140, compared with an average direct variable cost of $8,070 per case for patients whose treatment followed the protocol.
For patients who were treated under the appropriate order set, but still acquired a QVI, the average direct variable cost per case was $23,978, whereas for patients who were not treated under the appropriate order set and acquired a QVI, the average direct variable cost per case was $35,538. Thus, among patients who experienced a QVI, costs of care for those whose treatment complied with the appropriate core measure order set were significantly lower than for those whose treatment did not follow the standard protocol (p-value = 0.0008).
Sepsis: A Closer Look
The largest disparity between QVI rates, relative to order set compliance, was seen among patients qualifying for the sepsis core measure standard order set. Likewise, the largest discrepancies in average costs per case were seen among patients with sepsis.
The hospital identified nearly 2,200 inpatients qualifying for the sepsis core measure order set, of whom 31 percent received the appropriate order set. Of the 69 percent of patients whose treatment did not comply with the sepsis order set, 34 percent acquired one or more QVIs, with an average direct variable cost per case of $40,942. Meanwhile, of the 31 percent of patients whose treatment adhered to the core measure standard order set, 15 percent acquired one or more QVIs, with an average direct variable cost per case of $24,106. Thus, both the QVI rate and average direct variable cost per case for cases with one or more QVIs were lower for cases in which treatment followed the sepsis order set (p-values of < 0.0001 and 0.002, respectively).
The average direct variable cost per case for patients with a QVI, at $32,962, is significant compared with that without a QVI (i.e., $6,355). The data show that for patients with QVIs, on average, the length of stay (LOS) and cost per case were four to five times greater than for patients without QVIs.
Conclusion
By showing a significant difference in quality outcomes andcosts between patients who were treated under standard care protocols and patients who were not treated under the protocols, this study’s findings suggest there is value to be gained from continued usage and development of these standard order sets. The data suggest there is validity in long-held belief that standardizing processes improves outcomes for the patient and the hospital.
The findings also underscore the potential value of applying the lean methodology in a hospital setting. Standard order sets provide easy system navigation for physicians, resulting in less waste of physician’s time, better outcomes for patients, and reduced direct care costs for the hospital.
The data also suggest that hospitals have ample opportunity to use lean methods to develop and increase the adoption of standard order sets. In the case study described here, standard order sets were only used 30 percent of the time, presenting a significant opportunity for improvement. Senior executives should review the usage rates of standard order sets in their own organizations and seek to understand what types of barriers might exist that keep physicians from using these clinical tools. Key questions these executives ask include the following:
- Are the order sets up to date?
- Are the order sets easy to find and/or use in the electronic health record?
- Are physicians and residents aware that the order sets exist?
The study’s findings reinforce the view that promoting the usage of standard order sets constitutes a straightforward improvement initiative that correlates to lower costs and better patient outcomes.
As APMs become more prevalent, it will be incumbent on senior executives to be cognizant of all the various means available to their organizations for managing costs and reducing patient complications. Reducing complications by using standard care protocols, for example, allows hospitals to better manage patients after discharge and keep the cost of follow-up care low.
Data related to the cost of an episode of care are still in the early stages of being studied. Although such data continues to be developed and shared, hospitals executives should continue to look internally at how to reduce costs related to the initial anchor stay. Promoting the use of lean principles to develop standard care protocols and order sets and foster their widespread acceptance and use may be one of the most promising and effective places to start, with potential benefits in the form of both reduced costs and improved quality.